Overview
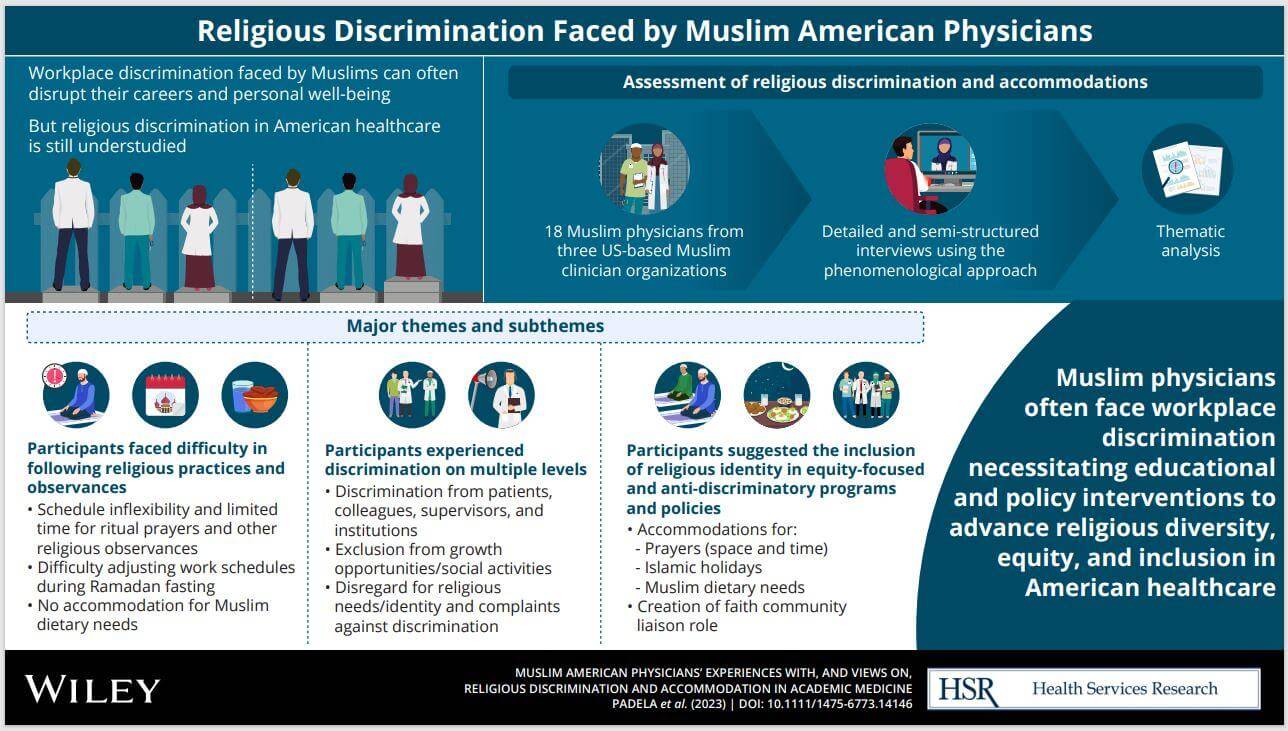
Workplace discrimination adversely impacts minority physicians’ career trajectories and well-being, and in so doing threatens health and healthcare equity. Although diversity, equity and inclusion programs have made great strides in countering discrimination based on gender, sexual and racial identity at the workplace, religious identities remain overlooked and understudied. Yet, religion is important to many physicians and aligning religious identity with one’s professional role can improve patient care and physician well-being. Muslim Americans are routinely subject to stereotyping, bias and discrimination. Drawing upon over a decade of research, these two national studies will reveal the impact of religious discrimination on the professional and psychological outcomes for Muslim physicians in the healthcare workplace. The 2013 study consisted of a quantitative survey, while the 2021 study involved both a survey and qualitative interviews, and across the two studies, there were a total of 519 participants (255 participants in 2013 and 264 participants in 2021).
Objectives
Quantify Muslim physicians’ experiences with religious discrimination
Compare trends between 2013 and 2021 national surveys
Examine Muslim physicians’ experiences with discrimination and accommodation, and identify barriers to the inclusion of Muslim physicians
Methodology
Since national databases of physicians, e.g., the American Medical Association Masterfile, do not collect religious affiliation, we obtained national samples of Muslim physicians by drawing upon membership rosters of national clinician organizations that explicitly integrate religious and professional identities in their organizational title and mission statements. In 2013, we drew a random sample from the Islamic Medical Association of North America (IMANA), the largest Muslim physician organization in the country. In 2021, our sample was recruited from American Muslim Health Professionals, the US Muslim Physician Network, as well as IMANA. Inclusion criteria for both surveys included being a practicing physician in the US, Muslim, and English literate. The 2021 study also required participants to presently work at a university-affiliated or academic medical center in the US or have worked at one within the past 20 years. Participants in the 2021 survey were also invited to participate in a semi-structured interview. The studies were approved by the Institutional Review Boards at the University of Chicago (2013) and the Medical College of Wisconsin (2021). All participants provided informed consent before enrollment in the respective studies.
Survey Participants
This section describes the 2013 and 2021 survey and interview participants. Notably, the 2013 study sample included 255 participants with a mean age of 52 years. The 2021 study sample comprised 264 participants and was significantly younger with a mean age of 39.5 years. In the 2013 study, 70% identified as South Asian, whereas in 2021, 33% identified as South Asian. Another statistically significant difference between the two include that the 2021 cohort had less years of medical practice. However, the gender composition of the two samples was similar (70% male in 2013, 65% male in 2021)
Interview Participants
When completing the 2021 survey, 186 participants met the eligibility criteria and indicated an interest in an interview. Of those participants, 18 were interviewed. The average age of interviewees was 41.5 years, and over half of the group (11/18) were female. Most of the participants interviewed were South Asian (13/18), and half (9/18) were born in the United States. To better situate their experiences in the context of the interviewees, a couple of survey items were used to categorize interviewees as experiencing either high religious discrimination or low religious discrimination; nine participants fell into each group. Similarly, they were categorized as experiencing either high religious accommodation or low religious accommodation; there were 12 participants in the first category and 6 participants in the second.
Results
Over the past 10 years, an increased number of Muslim physicians are experiencing religious discrimination, job turnover, and having patients refuse care.
- Workplace Discrimination
- Accommodations for Religious Identity
- Personal and Professional Impacts of Workplace Discrimination
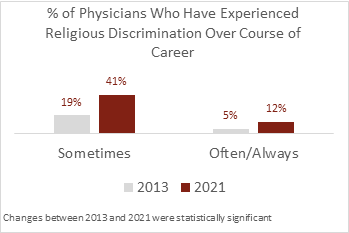
A greater proportion of Muslim physicians confront discrimination at work.
- In 2013, 19% of participants reported sometimes experiencing religious discrimination in the workplace, while 5% reported often or always encountering discrimination during their careers.
- In 2021, 41% of participants reported sometimes experiencing religious discrimination in the workplace, while 12% reported often or always experiencing discrimination.
A similar increase was seen in a question about participants’ current workplace:
- In 2013, 14% of participants reported currently experiencing religious discrimination at work.
- In 2021, 36% of participants reported currently experiencing discrimination at work.
Muslim physicians increasingly perceive that they have been passed over for professional advancement because of their religious identity.
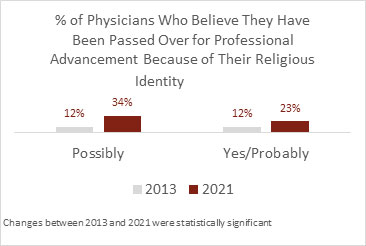
- In 2013, 24% of participants reported they have been passed over for professional advancement because of their religion.
- In 2021, 57% of participants reported that they have been passed over for professional advancement because of their religion.
In 2013, 24% of participants reported they have been passed over for professional advancement because of their religion.
In 2021, 57% of participants reported that they have been passed over for professional advancement because of their religion.
Interviewees echoed this phenomenon and shared specific instances. For example, a South Asian female physician stated:
In 2013, 9% of participants reported experiencing patient(s) refusing to be cared for by the participant due to the participant’s religious identity.
In 2021, 33% reported experiencing patient(s) refusing to be cared for by the participant due to the participant’s religious identity.
- In 2013, 9% of participants reported experiencing patient(s) refusing to be cared for by the participant due to the participant’s religious identity.
- In 2021, 33% reported experiencing patient(s) refusing to be cared for by the participant due to the participant’s religious identity.
Aside from being rejected by patients, participants also encountered discriminatory comments from patients; for example, a South Asian female interviewee reported that patients made comments such as:
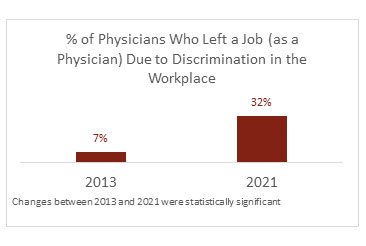
Muslim physicians are increasingly leaving their jobs due to workplace discrimination.
- In 2013, 7% of participants reported leaving a job due to discrimination.
- In the 2021 survey, 32% of participants reported the same.
Interview participants noted cumulative stress compelled them to leave. As one South Asian male participant shared:
Participants felt ‘accommodated’ through their own efforts at managing prayer or getting holidays covered by colleagues.
Almost three-fourths of respondents in both surveys (72% in 2013 and 76% in 2021 respectively) agreed with the statement that their workplace accommodates their religious identity. While this statistic appears encouraging, interviewees revealed that notions of accommodation focused on their own initiatives rather than the institutional outreach. This ‘self-accommodation’ may have started at the beginning of their careers with their choice of specialty. As one Arabic female interviewee noted:
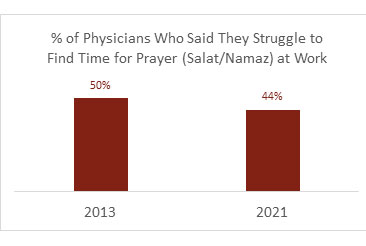
Nearly half of respondents struggled to find time for prayer at work.
Prayer Accommodations
Muslims are obligated to pray five times a day during certain time slots. Each prayer takes about five minutes, and several prayer times fall within a standard workday. About half of respondents on each survey said they struggled to find time to pray at work.
One South Asian male participant explained how he managed prayer time into his workday:
Accommodations for Islamic Dress and Appearance
Islamic identity is also connected to dress and appearance. Aside from modest dress, Muslim men may wear a beard as it is highly recommended religious practice, while Muslim women may wear a ḥijāb (a headscarf) or niqāb (face covering) as part of their commitment to religious mores. Wearing the ḥijāb in sterile environments was particularly difficult in the absence of institutional guidelines. A South Asian female participant shared her practice:
On the other hand, one South Asian male participant decided to avoid all criticism from colleagues who perceived beards to be unprofessional by deciding not to have beard altogether as it “will draw more attention.”
Accommodations for Religious Holidays and Ramadan fasting
Interview participants identified several challenges related to work schedules and Ramadan fasting, as well as the Eid holidays. Ramadan occurs during the ninth month of the Islamic calendar, and is marked by obligatory ritual fasting, e.g., abstaining from food, drink and sexual intimacy, from dawn to dusk. It also includes special nightly prayer vigils held at mosques. Fasting can be physically demanding, and some physicians might require less demanding clinical schedules especially when Ramadan falls in summer months. Two principal holidays mark the Islamic calendar. Eid al-Fitr is the celebration directly following Ramadan and consists of special congregational prayers in the morning. Eid al-Adha, on the other hand, is contemporaneous to the obligatory religious pilgrimage to Mecca, the Hajj. That holiday is also marked by special congregational prayers in the morning as well as ritual sacrifice. As with any holiday, these days are celebrated with friends and family. Participants shared that adjusting clinical schedules and securing time off posed some challenges.Illustrating the issue, one South Asian female participant reflected that he could never be sure to get his work schedule adjusted despite asking for accommodation:
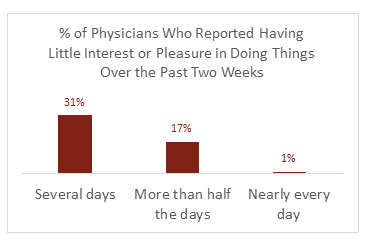
In the 2021 study, participants reported symptoms of depression and burnout.
- In the 2021 survey, 49% of participants reported having little interest or pleasure in doing things over the past two weeks.
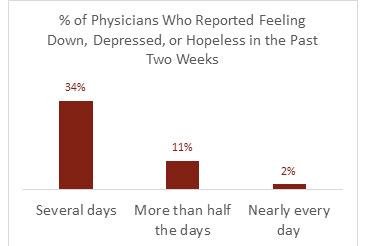
- On the 2021 survey, 47% of participants reported feeling down, depressed, or hopeless in the past two weeks.
- Twenty-one percent of participants screened positive for depression.
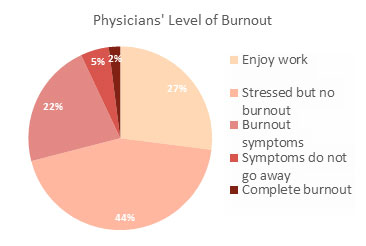
- On the 2021 survey, 29% of participants stated they were feeling some degree of burnout and had one or more symptoms of burnout, such as physical or emotional exhaustion.
Interview participants further clarified the psychological and health toll of workplace discrimination. Out of the 18 participants, 12 feared revealing their religious identity; 10 harbored stress due to microaggressions; and 10 experienced depression/anxiety. As one South Asian female interviewee noted, their religious identity put them at risk:
Project Timeline
Interview participants from our 2021 study provided specific recommendations for how their religion could be better accommodated at work:
The most overarching need voiced by participants was for education and for policy intervention. They noted how diversity, inclusion, and equity programming largely overlooked the religious dimensions of physician identity, and as such Muslims did not have a platform through which to engage colleagues and leaders over their experiences. Healthcare systems needs to include religious identity within the scope of diversity, equity and inclusion initiatives and the accompanying data dashboards. Educational programs directed at all levels of the workforce that center Muslim identity would create awareness of the challenges and needs of this group. At the same time, policy interventions are required. Many healthcare systems do not directly address religious accommodations; there are no policies to facilitate time off to pray nor guidelines covering accommodations for religious garb. Participants shared that those written policies could reduce the burden they face in trying to obtain accommodations. Beyond these overarching recommendations, the following were suggested:
- Providing support and designated spaces for daily and Friday prayer.
- Acknowledging the practice of Ramadan fasting and Islamic holidays.
- Creating policies to protect Muslim dress code in the workplace.
- Recognizing Muslim dietary preferences and restrictions.
- Instituting a faith community liaison position.
- Medical education should account for religious identity.
Healthcare systems must mitigate religious discrimination and promote accommodation through a multi-tiered and systematic approach. The following research and evidence offers several data-driven strategies for addressing the needs of Muslim physicians in the healthcare workforce.
Summary and Implications
Discrimination and bias directed at Muslims in American society emerges from a complex array of factors including the rise in racial and religious prejudice, overwhelming negative portrayals of Muslims in political discourse and popular media, a general lack of awareness of Muslim beliefs and values among the populace. This societal climate spills over into religious discrimination and lack of accommodation in healthcare for both patients and providers. Muslim physicians in the US suffer from workplace discrimination directed at their religious identity, and these negative experiences may be increasing. Comparisons between the two surveys reveal several statistically significant changes in that a higher proportion of physicians in 2021 than in 2013 report experiencing religious discrimination over their career course (24% to 53%), having left a job due to such discrimination (7% to 32%), and having patients refuse their care (9% to 33%) due to their religious identity. Additionally, almost half of respondents in each survey struggled to perform obligatory ritual prayer at work. In the 2021 survey, nearly half reported having little to no interest in doing things (48%) or feeling depressed (47%) during several or more days within the past 2 weeks, and 29% of participants stated they were experiencing burnout. Finally, the interviews from the 2021 study revealed additional barriers to the inclusion of Muslim physicians in medicine. In the absence of policies and a culture of proactive accommodation, clinicians used self-management strategies to maintain religious practices and observances.
These studies highlight how religious identity and religiosity negatively impact workplace experiences and well-being among Muslim physicians in healthcare and highlights the deep psychological and career effects of working in a space perceived to be non-accommodating of religious practices. Healthcare workforce diversity, inclusion, and equity programming should include a focus on accommodating the religious identities of physicians.
Policy Report
Publications
- Religious Identity Discrimination in the Physician Workforce: Insights from Two National Studies of Muslim Clinicians in the US, J Gen Intern Med,2022.
- The Impact of Practicing Both Medicine and Religion: Muslim Identity as a Predictor of Discrimination, Accommodation, and Career Outcomes in Academic Medicine, Academic Medicine,2022.
- Career Satisfaction and Burnout among American Muslim Physicians, Avicenna Journal of Medicine 2023.
- Muslim American physicians’ Experiences With, and Views on, Religious Discrimination and Accommodation in Academic, Health Science Research, 2023.
- A religious minority tax in healthcare? Insights from Muslim American physicians, Qualitative Research in Health.
Presentations
Community Conferences
- Muslim Clinicians in the Medical Academy, Anesthesiology Grand Rounds DEI, Medical College of Wisconsin, Milwaukee, WI, 2/2022.
- Being Muslim in Academic Medicine, Nagamia Institute of Islamic Medicine and Sciences (NIIMS), Rolling Meadows, IL, 7/2022.
- Accommodating Muslim Values in Healthcare, Medical College of Wisconsin, Milwaukee, WI, 8/2022.
- Health Policy & Advocacy Priorities for American Muslims Centering Equity, National American Muslim Policy Conference, Virtual, 6/2022.
- Advancing Equity for Muslim Physicians in the Healthcare Workforce, 31st Annual Wisconsin Emergency Medicine Research Forum, Madison, WI, 3/2023.
Academic Conferences
- Religious Identity Discrimination in the Physician Workforce: Insights from Two National Surveys of Muslim Clinicians in the US, Conference on Medicine and Religion, Portland, OR, 3/2022.
- Religious Accommodation or Professional Indoctrination? Experiences of Muslim Physicians in Academic Medicine, Conference on Medicine and Religion, Portland, OR, 3/2022.
- Advancing Institutional Workforce Equity: Insights From Muslim Physicians in Academic Medicine, The Academy for Professionalism in Health Care, Philadelphia, PA, 6/2022.
- Religiosity Predicts Discrimination, Accommodation, and Career Outcomes for Muslim Physicians in Academic Medicine, The Academy for Professionalism in Health Care, Philadelphia, PA, 6/2022.
- Religious Identity Discrimination in the Physician Workforce: Insights from Two National Surveys of Muslim Clinicians in the US, American Muslim Medical Students Association, Ann Arbor, MI, 8/2022.
Media Highlights
- Washington Post.
- Discrimination Against Muslim Physicians on the Rise, Advancing Equity for Muslim Physicians in the Healthcare Workforce.
- Muslim physicians report significant discrimination, March,1/ 2023.
- The Detroit News.
- Medical College of Wisconsin Research Shows Increasing Religious Discrimination Against Muslim Physician In U.S, Jan,4/ 2022.
- Corewell Health Clinic Accused of Religious Discrimination, Overprescribing Opioids, March,26/2023.
- Whitehead, S. (2023). Muslim Physicians Face Rising Discrimination, Islamic Horizons Journal, March,01/2023.
Links to Resources
- Know Your Rights – A fact sheet describing religious rights in the workplace and what steps to take if your rights have been disregarded, Muslim Advocates.
- Filing a Conscience and Religious Freedom Complaint – File a complaint online about religious discrimination. Federal Conscience and Religious Freedom Laws help to protect you from coercion, discrimination on the basis of conscience or religion, and burdens on the free exercise of religion, Office of Civil Rights.
- Ḥijāb in the OR – A guide to ḥijāb in the operating room, written by Dr. Deena Kishawi.
Employee Resources:
- An Employer’s Guide to Islamic Religious Practices – A pamphlet designed to aid employers in formulating and implementing policies to create a culturally inclusive workplace, Council on American-Islamic Relations.
- Religious Diversity Manager Training – A session designed for managers to learn how to respond to accommodation requests and foster an inclusive work environment, Tanenbaum Foundation.
- TAHSN Standards for Religious Attire for Health Care Workers, Learners and Volunteers in Hospital Areas with Sterile Procedure – Standards and shared expectations related to clothing worn by religiously observant individuals working in hospital areas with sterile procedures, The Toronto Academic Health Science Network (TAHSN)
- Muslim Resident Cases – A chapter in the book, Diversity and Inclusion in Quality Patient Care: A Case-Based Compendium (pgs. 305-314), that presents four cases of ethical challenges in healthcare provision for Muslim patients.
Other Dissemination Activities:
- Article: Religious Identity Discrimination and Accommodation Experienced by Muslim American Physicians in Academic Medicine.
- PodCast: Religious Discrimination and Accommodation of Clinicians in Academic Medicine, Healthcare Professionalism: Education, Research & Resources.
Dissemination Products




Videos
Discrimination & Diversity in Healthcare Workforce
Aasim Padela, MD, MSc - Religion
Being Muslim in Academic Medicine
Healthcare Workforce Webinar
- Funding
- Partner Organizations
- Co-publishing organizations:

The opinions expressed in this publication are those of the authors. They do not reflect the opinions or views of the grant funding organizations.



Gallery


Meet The Project Team
Aasim I. Padela, MD, MSc
(Medical College of Wisconsin & The Initiative on Islam and
Medicine)

Laila Azam, PhD, MBA
Medical College of Wisconsin
Research Scientist

Benish Baqai
Medical Student at the Medical College of Wisconsin

Sohad Murar , PhD
Research Scientist